
| |
 | A Patient's Guide to Carpal Tunnel
Syndrome
|
Home

| Introduction
|
Carpal tunnel syndrome is a common problem that affects the hand and
wrist. This condition, or syndrome, has become the focus of much attention in the
last few years due to suggestions that it may be linked to occupations that require
repetitive use of the hands - such as typing. In reality, there are many people who
develop this condition - regardless of the type of work which he or she does.
The following documents attempt to explain what carpal tunnel
syndrome is, how it is diagnosed, and describe the treatment options available.
| Anatomy
|
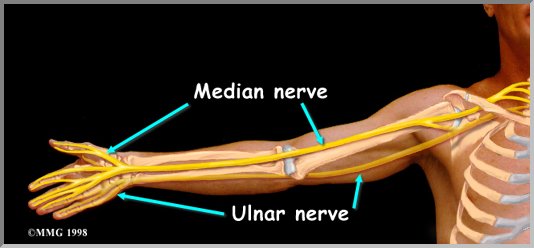
| The Median Nerve
Carpal tunnel syndrome (CTS) is a condition which results
when the median nerve does not work properly. Usually, this is thought to occur
because there is too much pressure on the nerve as it runs into the wrist through an
opening called the carpal tunnel. It may be easier to understand how this
occurs if you understand some of the anatomy of the wrist. The median nerve runs
into the hand to supply sensation to the thumb, index finger, long finger, and half of the
ring finger. The nerve also supplies a branch to the muscles of the thumb, the
thenar muscles. These muscles help move the thumb and are very important in
moving the thumb so that you can touch each of the other fingers. This motion is
called opposition.
The carpal tunnel is an opening into the hand that is made up
of the bones of the wrist on the bottom and the transverse carpal ligament on the
top. Looking at a cross section of the wrist allows one to visualize the
anatomy of the carpal tunnel. Through this opening called the carpal tunnel, the median
nerve and the flexor tendons runinto the hand. Looking a little closer, we see that the
median nerve lies just under the transverse carpal ligament.
The flexor tendons are important because they allow us to move the
fingers and the hand, such as when we grasp objects. The tendons are covered by a
material called tenosynovium. The tenosynovium is very slippery, and allows the tendons to
glide against each other as the hand is used to grasp objects. Any condition which
causes irritation or inflamation of the tendons can result in swelling and thickening of
the tenosynovium. As the tenosynovium covering all of the tendons begin to swell and
thicken, the pressure begins to increase in the carpal tunnel - because the bones and
ligaments that make up the tunnel are not able to stretch in response to the
swelling. Increased pressure in the carpal tunnel begins to squeeze the median nerve
against the transverse carpal ligament - because the nerve is the softest structure in the
carpal tunnel. Eventually, the pressure reaches a point when the nerve can no longer
function normally. Pain and numbness in the hand begins.
One of the first symptoms of carpal tunnel syndrome is numbness in
the distribution of the median nerve. This is quickly followed by pain in the same
distribution. The pain may also radiate up the arm to the shoulder, and, sometimes
the neck. If the condition is allowed to progress, weakness of the thenar muscles
can occur. This results in an inability to bring the thumb into opposition with the
other fingers and hinders one's grasp.
There are many conditions which can result in irritation and
inflammation of the tenosynovium, and eventually cause carpal tunnel syndrome.
Different types of arthritis can cause inflammation of the tenosynovium directly. A
fracture of the wrist bones may later cause carpal tunnel syndrome if the healed fragments
result in abnormal irritation on the flexor tendons. The Key Concept to remember is
that anything which causes abnormal pressure on the median nerve will result in the
symptoms of pain, numbness and weakness of carpal tunnel syndrome. Recently, physicians
have begun to recognize that activities that involve highly repetitive use of the hands
can result in carpal tunnel syndrome. This is thought to be caused by inflammation
and swelling of the tenosynovium due to overuse.
|
| Diagnosis
Evaluation begins by your doctor obtaining a history of the problem,
followed by a thorough physical examination. Your description of the symptoms and
the physical examination are the most important parts in the diagnosis of carpal tunnel
syndrome. Commonly, patients will complain first of waking in the middle of
the night with pain and a feeling that the whole hand is asleep. Careful
investigation usually shows that the little finger is unaffected. This can be
a key piece of information to make the diagnosis. If you awaken with your hand
asleep, pinch your little finger to see if it is numb also, and be sure to tell your
doctor if it is or isn't. Other complaints include numbness while using the hand for
gripping activities, such as sweeping, hammering, or driving. The major physical
findings reflect that pressure is increased in the carpal tunnel.
If more information is needed to make the diagnosis, electrical
studies of the nerves in the wrist may be requested by your doctor. Several tests
are available to see how well the median nerve is functioning, including the nerve
conduction velocity (NCV). This test measures how fast nerve impulses are conducted
through the nerve.
|
| Treatment
|

| Non-Operative Treatment
|
In the early stages of carpal tunnel syndrome, a simple brace will
sometimes decrease the symptoms, especially the numbness and pain occurring at
night. These braces simply keep the wrist in a neutral position (not bent back too
far nor bent down too far). When the wrist is in this position, the carpal tunnel is
as big as it can be - so the nerve has as much room as possible. The brace needs to
be worn at night while you sleep to prevent the numbness and pain occurring at
night. If you have symptoms during the day as well, the brace may help reduce those
symptoms as well.
Anti-inflamatory medications may also help control the swelling of
the tenosynovium and reduce the symptoms of carpal tunnel syndrome. These
medications include the common over the counter medications such as ibuprofen and
aspirin. In some studies, high doses of Vitamin B-6 have also shown some
efficacy in decreasing the symptoms of carpal tunnel syndrome.
There is some evidence that exersises may prevent or control the
symptoms of carpal tunnel syndrome. Another good discussion of the technical aspects
of the reducing the riscs of carpal tunnel syndrome suggests that wrist problems may
contribute to the problem. Workplace ergonomics have long been thought to be a
contributing factor and alteration of the worksite is a must for patients doing any type
of repetitive work.
If these simple measures fail to control your symptoms an injection
of cortisone into the carpal tunnel may be suggested. This medication will decrease
the swelling of the tenosynovium and may give temporary relief of symptoms. It
is used not only to treat the problem, but serves to aid in diagnosis. If you don't
get even temporary relief from the injection, it may be a sign that other problems exist
that are causing the carpal tunnel symptoms. There is also a newer way
to get cortisone medications down into the carpal tunnel. Iontophresis is a
technique where an electrical current is used to move the molecules of the medication
through the skin down into the carpal tunnel. It is less painful than an injection,
but is probably not as effective.
| Surgical Treatment
If all of the previous treatments fail to control the symptoms of
carpal tunnel syndrome, surgery may be required to reduce the pressure on the median
nerve. There are several different surgical procedures designed to relieve pressure
on the median nerve. The most common are the traditional open incision technique
described below, and the newer Endoscopic Carpal Tunnel Relise using a smaller incision
and a fiberoptic TV camera to help see inside the carpal tunnel.
|
| Basic Steps in Open Carpal Tunnel Release
|
Step 1 A small incision, usually less than 2 inches, is made
in the palm of the hand. In some severe cases, the incision needs to be extended into the
forearm another 1/2 inch or so.
Step 2 After the incision is made through the skin, a
structure called the palmar fascia is visible. An incision is made through this material
as well, so that the constricting element, the transverse carpal ligament, can be seen.
Step 3 Once the transverse carpal ligament is visible, it is
cut with either a scalpel or scissors, while making sure that the median nerve is out of
the way and protected.
Step 4 Once the transverse carpal ligament is cut, the
pressure is relieved on the median nerve.
Step 5 Finally, the skin incision is sutured. At the end of
the procedure, only the skin incision is repaired. The transverse carpal ligament remains
open and the gap is slowly filled by scar tissue.
A bulky dressing is applied to the hand following
surgery. You should leave this in place until your first office visit after
the surgery. Your sutures will be removed 10 - 14 days after surgery.
You should avoid any heavy use of the hand for 4 weeks after your surgery. You
should not get the stitches wet. Expect the pain and numbness to begin to improve
after surgery, but you may have tenderness in the area of the incision for several months.

The information
provided here is not meant to take the place of the complete exam by a physician. If you
have an injury we strongly encourage you to get adequate medical care
Home |